
I’m consulting with a man in his mid 70s: a retired teacher in an inner city secondary school. He used to smoke, but quit several years ago. He’s otherwise pretty fit: he has never learned to drive so walks everywhere and uses public transport. He is married, and his wife and he are still independent. They have grown up children who live a long way away. They go out to the theatre when they can and enjoy going to the local pub together and with friends. He’s got high blood pressure which is well controlled. He also has an abdominal aortic aneurysm (an AAA). It’s large. And he is worried about it. We talk about the options for repair. He is anxious about a major abdominal operation. He’s not dead set against it, but is concerned about the recovery, the impact it will have on his wife. On balance he is minded to have an endovascular repair, for which the AAA is anatomically suitable. We discuss the long term outcomes of open and endovascular repair. The need for secondary procedures and surveillance. He leaves the consultation undecided and plans to discuss it with his family.
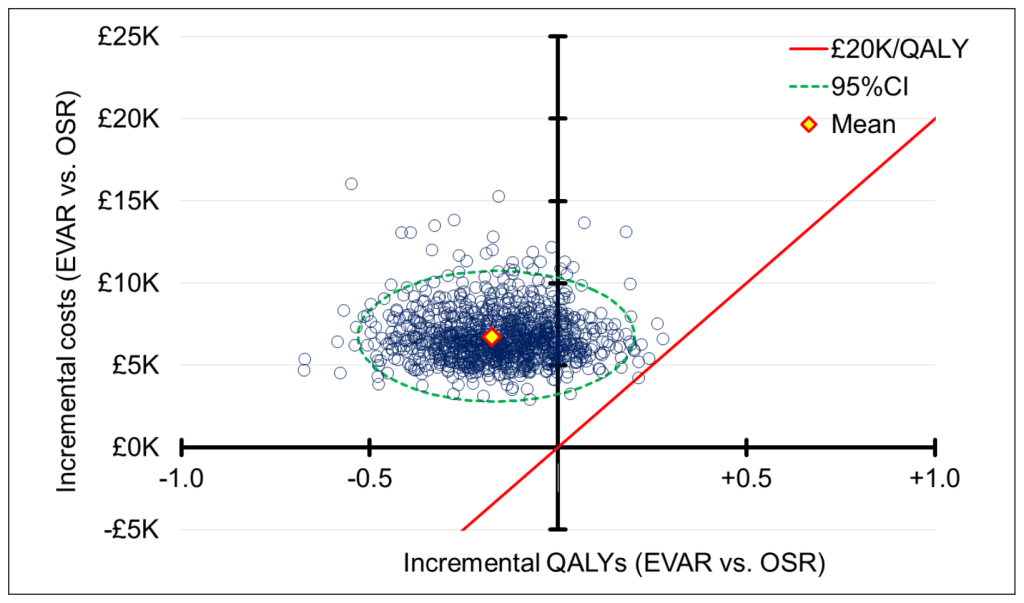
I have spent the last 5 years on the NICE Guideline Development Committee, developing a guideline for the management of people with AAA. The results of several large trials comparing open and endovascular repair of AAA are consistent that while endovascular repair and open repair are safe (meaning very few people die from them), endovascular repair is safer by a small margin and gets people out of hospital and back to normal substantially more quickly than open surgery. However the longer term outcomes are not as good and beyond about 7 years, more people are dead after endovascular repair than after open repair. Because of this, endovascular repair is not cost effective, meaning the opportunity cost of providing it is too great and at a population level offering endovascular repair causes harm. Putting aside arguments about the contemporary relevance or methodological detail of the evidence, the only possible conclusion is that endovascular repair should not be undertaken if someone can have an open operation.
There are several problems with accepting this analysis. One is that it requires a belief that savings made in one place in the healthcare economy will be realised in a benefit elsewhere: something called Pareto efficiency. This might be an intellectual leap too far for some in the NHS of 2020. But perhaps the biggest issue that it is a cold joyless analysis – a faceless functional accounting, the reduction of individual encounters to marks on a Kaplan-Meier chart. It is the science in medicine, but medicine is more than science. It’s an art. For me some of the joy of practicing medicine is in this art: the ability to synthesise the evidence into a narrative a patient can engage with, helping them work out the best option. What do I do then, when having done this, my patient’s preferred option is not cost effective, when the art and the science collide? How do I decide between the interests of a real person sitting before me, vulnerable, perhaps anxious, who trusts me to make decisions with them, for them and in their best interests and the interests an unknown person (or group) with whom I have no relationship – the people who will theoretically benefit if I choose the science over the art. How do I decide between my patient and society?
Since the publication of the draft NICE guidance on AAA, which recommended against endovascular repair partly on the basis of cost effectiveness arguments, I have defended and explained the decisions the guideline committee made at conferences, in conversations and in print. I have posed questions to conference panellists who were challenging the guideline about whether they think cost effectiveness is an important consideration when deciding a therapy and received frequently unconvincing responses. But in the back of my mind, I’m questioning: are they right? Are the unseen consequences of my clinical decisions (for unknown people) my responsibility or are these too distant from me to consider.
Within the contexts by which NICE asks its committees to make decisions, the answer is clear: they are not too distant, and must be taken into account. But while it may be the right thing to do, to follow the science and deny treatments that are not cost effective, it can feel wrong. It’s a depressing analysis to frame the future for individual people in terms of population outcomes. Individual characteristics, ambitions, concerns and expectations, love, beauty and hope are subordinated to the inevitable logic of the data. This feels like a betrayal of the doctor-patient relationship which is ultimately a personal one: and guidelines are implemented at a personal level, patient by patient.
This is not a new dilemma, either in medicine or in economics in general. It is a version of ‘the tragedy of the commons’. To some extent patients, the public and physicians understand it, in the general acceptance of triage in emergency departments, or waiting lists for elective treatment. But the idea of not offering treatments at all, solely on the basis of a cost effectiveness calculation, seems to be too much for many people in their role as clinicians or patients, even if it makes sense in their role as taxpayers. In fact it is probably impossible (and certainly not desirable) for clinicians to make bedside judgements on the basis of cost effectiveness, not only because of how it makes them feel, but also because it would undermine the trust central to the relationship with their patient. Solutions to the dilemma attempt to constrain the options available to clinicians either by incentivising certain therapies, or by limiting choice to cost effective options only (by either not funding the alternatives or by creating guidelines). In order to allow these solutions, clinicians need to accept that some decisions are taken out of their hands. But in doing this, it can seem as if the art in their practice is reduced to a near irrelevance. Perhaps this, then, is one of the reasons for the criticism, even resentment, of some of NICE’s draft AAA guidance.
Where does this leave us? We are caught in the cleft stick of increasingly costly technological advances in healthcare, wanting to offer them to our patients where appropriate, but understanding that ultimately resources are finite. We will need to face this as a society and as individual clinicians sooner or later unless healthcare costs are to escalate uncontrollably. We surely need to understand that the technical advances that interest us may not be in the best interests of society at large, and accept this where it is the case. We need to allow trusted organisations to make these decisions for us, within an open and transparent process, and we need to allow that the art in medicine (and our joy in practising it) is retained but refocussed to help our patients navigate their therapy choices within the constraints imposed on us by those trusted organisations. NICE’s failure to stand firm on its principles in respect of this aspect of the AAA draft guidance sets an unfortunate precedent and makes these issues more difficult, not less.
My patient returns to clinic. He has spoken with his family and his wife. He wants an endovascular repair. Cognitive dissonance rages within me. I take a deep breath in, and begin….

You must be logged in to post a comment.